-
Ever wanted an RSS feed of all your favorite gaming news sites? Go check out our new Gaming Headlines feed! Read more about it here.
-
We have made minor adjustments to how the search bar works on ResetEra. You can read about the changes here.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Is there a source besides this tweet that is saying 40%. WHO needs to fire their entire Comms team.
Video here. Starts at 01:22 or so:

#COVID19 LIVE Q&A with Dr Mike Ryan and Dr Maria Van Kerkhove - #AskWHO of 9 June 2020
#AskWHO series: This was the live discussion about the COVID-19 pandemic of 9 June 2020 with Dr Mike Ryan, Executive Director of WHO Health Emergencies Progr...
 youtu.be
youtu.be
Awesome thanks!Video here. Starts at 01:22 or so:
#COVID19 LIVE Q&A with Dr Mike Ryan and Dr Maria Van Kerkhove - #AskWHO of 9 June 2020
#AskWHO series: This was the live discussion about the COVID-19 pandemic of 9 June 2020 with Dr Mike Ryan, Executive Director of WHO Health Emergencies Progr...
Finland today:
So far the infection rate hasn't went up despite restrictions being lifted.
Outdoor sports events (baseball, soccer) are starting this week, with a restriction of 500 spectators.
Next month it will be 500 spectators per stand, each stand needs to have separate entry/exit and other facilities. So depending on the stadium size each event will have a capacity of around 500 to 3000.
- 24 new cases
- 1 new death
- 4 in ICU (total)
- 28 in hospital (total)
So far the infection rate hasn't went up despite restrictions being lifted.
Outdoor sports events (baseball, soccer) are starting this week, with a restriction of 500 spectators.
Next month it will be 500 spectators per stand, each stand needs to have separate entry/exit and other facilities. So depending on the stadium size each event will have a capacity of around 500 to 3000.
Regarding the WHO and asymptomatic transmission.
I have listended to both yesterday's and today's explanation. And there is a clear distinction they made: Contract tracing and models.
While doing contact tracing it seems rare that an asymptomatic person could spread the virus. This is what several countries seem to report and based on actual contract tracing data. That information is not perfect, but at least helpful as an additional data point. Contract tracing asymptomatic persons seems to be a pain honestly and probably a reason why there are not many studies yet.
On the other hand, there are models that estimate the proportion of asymptomatic transmitters at 40%, with a high range of uncertainty.
And they mentioned, yesterday and today, that the data is not conclusive and that they cannot fully answer the question and need more research.
And that's being done.
I have listended to both yesterday's and today's explanation. And there is a clear distinction they made: Contract tracing and models.
While doing contact tracing it seems rare that an asymptomatic person could spread the virus. This is what several countries seem to report and based on actual contract tracing data. That information is not perfect, but at least helpful as an additional data point. Contract tracing asymptomatic persons seems to be a pain honestly and probably a reason why there are not many studies yet.
On the other hand, there are models that estimate the proportion of asymptomatic transmitters at 40%, with a high range of uncertainty.
And they mentioned, yesterday and today, that the data is not conclusive and that they cannot fully answer the question and need more research.
And that's being done.
I remember reading something from CDC saying that infection was less likely to occur with objects. Anyone have an update on that? Mostly interested to know how safe is it to order stuff and have them delivered home.
Looks like it's official...my family is all going back to work in some capacity next week, which means my daughter is going back to preschool. All in the NY/NJ area. Not thrilled, but I guess it was inevitable. Makes me wish I made enough money to sustain the fam until we're truly safe, but alas.
Has anyone else here been reintegrating? How's it going? The thing I'm most concerned about is sending my daughter back to preschool to be honest.
Has anyone else here been reintegrating? How's it going? The thing I'm most concerned about is sending my daughter back to preschool to be honest.
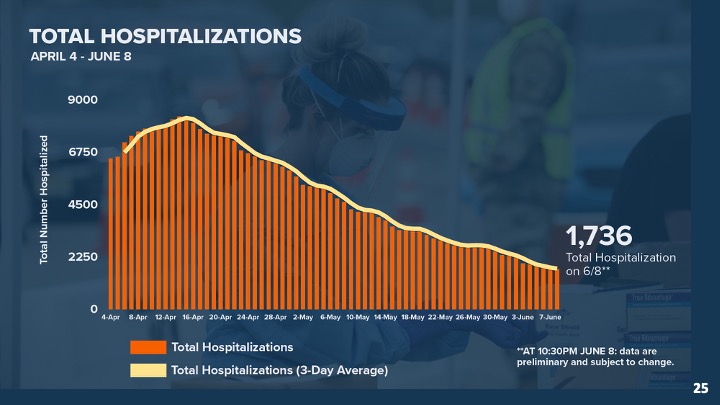
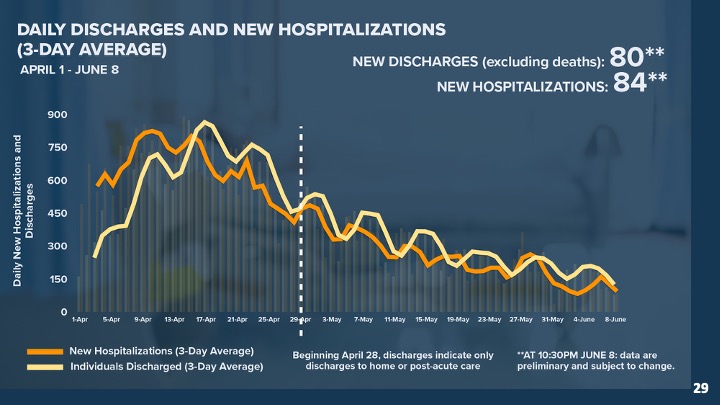
NJ Daily Numbers:
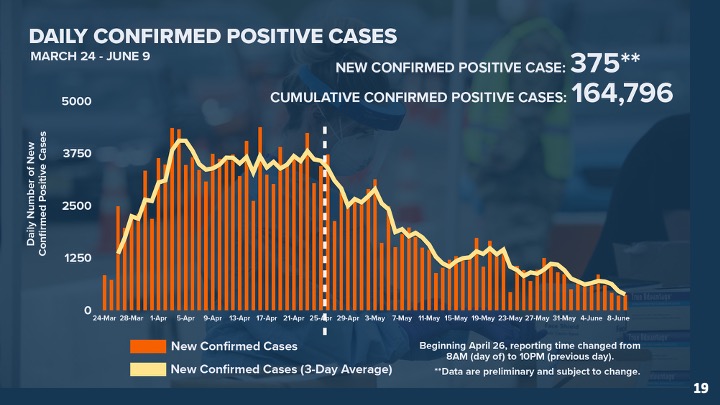
+375 new cases (164796 total)
+91 deaths (12303 total)
3 Massive Re-Opening items today:
Shelter in place is being lifted today via Executive Order.
Indoor gatherings are now allowed at either 25% of capacity or less than 50 people WITH face coverings.
Outdoor gatherings are now allowed up to 100 people. Exceptions are made for protests and "1st amendment activities"
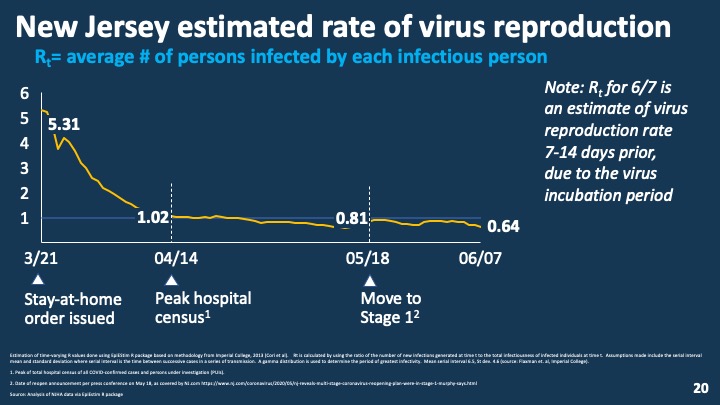
R0 is at 0.64 which is awesome
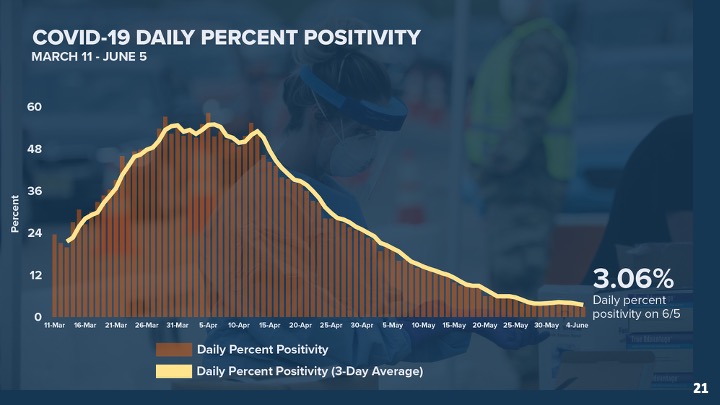
Positivity almost at 3%
+375 new cases (164796 total)
+91 deaths (12303 total)
3 Massive Re-Opening items today:
Shelter in place is being lifted today via Executive Order.
Indoor gatherings are now allowed at either 25% of capacity or less than 50 people WITH face coverings.
Outdoor gatherings are now allowed up to 100 people. Exceptions are made for protests and "1st amendment activities"
R0 is at 0.64 which is awesome
Positivity almost at 3%
In the greater NYC area, the virus is dieing out rapidly (look at my post right below yours) and we have the proper testing infrastructure in place now. The risk isn't completely eliminated but its minimal. Now if you were in Texas or Florida I'd be REALLY worried.Looks like it's official...my family is all going back to work in some capacity next week, which means my daughter is going back to preschool. All in the NY/NJ area. Not thrilled, but I guess it was inevitable. Makes me wish I made enough money to sustain the fam until we're truly safe, but alas.
Has anyone else here been reintegrating? How's it going? The thing I'm most concerned about is sending my daughter back to preschool to be honest.
I think when things are calm they need a thorough accounting of all their mistakes, misfires, and blunders and multiple heads should roll. Hopefully Biden is elected and the US again funds it as well as there is clearly a role for an effective WHO (as opposed to the borderline incompetent one we seem to have).
In the greater NYC area, the virus is dieing out rapidly (look at my post right below yours) and we have the proper testing infrastructure in place now. The risk isn't completely eliminated but its minimal. Now if you were in Texas or Florida I'd be REALLY worried.
'Minimal risk' is a big statement. But it certainly seems like people are acting based on that assumption. I'm in Manhattan and people are acting like it's a regular day in June.
Minimal risk with the proper precautions is the better way to put it.'Minimal risk' is a big statement. But it certainly seems like people are acting based on that assumption. I'm in Manhattan and people are acting like it's a regular day in June.
'Minimal risk' is a big statement. But it certainly seems like people are acting based on that assumption. I'm in Manhattan and people are acting like it's a regular day in June.
Yes, the virus is still out there. I don't want to be the person that gets it or gives it to someone vulnerable. I'm lucky in that my work quickly switched to WFH (since March 11th here in NJ) and they are in no hurry to open the office up. Sounds like they might make it a permanent thing.
I'm mostly happy with how NJ is handling it, but I expect my fellow residents to let their guards down. Indoor capacity of 50 people is dumb, ain't no way they are enforcing masks at offices and such. If we can make it to the end of July and there is no spike, then I will finally feel comfortable (still will take precautions). Then in the Fall I'll start feeling a little leery again. Can't imagine going to get my haircut for a long time.
In the greater NYC area, the virus is dieing out rapidly (look at my post right below yours) and we have the proper testing infrastructure in place now. The risk isn't completely eliminated but its minimal. Now if you were in Texas or Florida I'd be REALLY worried.
Thanks for posting the details. I'm still concerned and just facing the reality that we've gotta get back out there without knowing if/when there will be another spike/wave.
NJ Daily Numbers:
+375 new cases (164796 total)
+91 deaths (12303 total)
3 Massive Re-Opening items today:
Shelter in place is being lifted today via Executive Order.
Indoor gatherings are now allowed at either 25% of capacity or less than 50 people WITH face coverings.
Outdoor gatherings are now allowed up to 100 people. Exceptions are made for protests and "1st amendment activities"
Alright fellow New Jerseyans, let's not screw this up please!
Was talking to my mother and she was like if we can all just keep washing our hands and wear masks we might have a nice August lol
Has this been posted yet:

 www.cnn.com
www.cnn.com
More than half of states may be undercounting coronavirus cases by not following CDC guidelines
More than half of states may be undercounting coronavirus cases by not following CDC guidelines
At least 28 states are not following US Centers for Disease Control and Prevention guidelines on reporting new Covid-19 cases -- half of which saw the trend of new cases increasing in the last week.
More than half of states may be undercounting coronavirus cases by not following CDC guidelines
At least 28 states are not following US Centers for Disease Control and Prevention guidelines on reporting new Covid-19 cases -- half of which saw the trend of new cases increasing in the last week.
lol, I think she might be right, things are looking really positiveAlright fellow New Jerseyans, let's not screw this up please!
Was talking to my mother and she was like if we can all just keep washing our hands and wear masks we might have a nice August lol
Moscow Lifts Lockdown Restrictions Amid Virus Concerns
Moscow emerged from a strict lockdown Tuesday with the city government citing a slowdown in the coronavirus outbreak and critics expressing concerns over the potential for a new wave of infections in the Russian capital.
Moscow Lifts Lockdown Restrictions Amid Virus Concerns
CT reported less than 100 new cases today, for the first time since testing was put in place. But they also reported less than 5000 tests performed, which is a lower daily number than it has been. So this low positivity could still be a blip, but we'll see. Two weeks after memorial day and 20 days after the state "reopened", no bump in cases or hospitalizations so far.
Bulletin for the
French situation for the 09/06:
154591 confirmed cases + 403 in 24H
hospital:
11961 hospitalized -354 in 24 H (169 entries)
955 in intensive care -69 in 24 H (15 entries)
18912 dead + 53 in 24 H
Care homes:
37599 cases +194
10384 dead + 34
Total 29296 deaths +87 in 24H
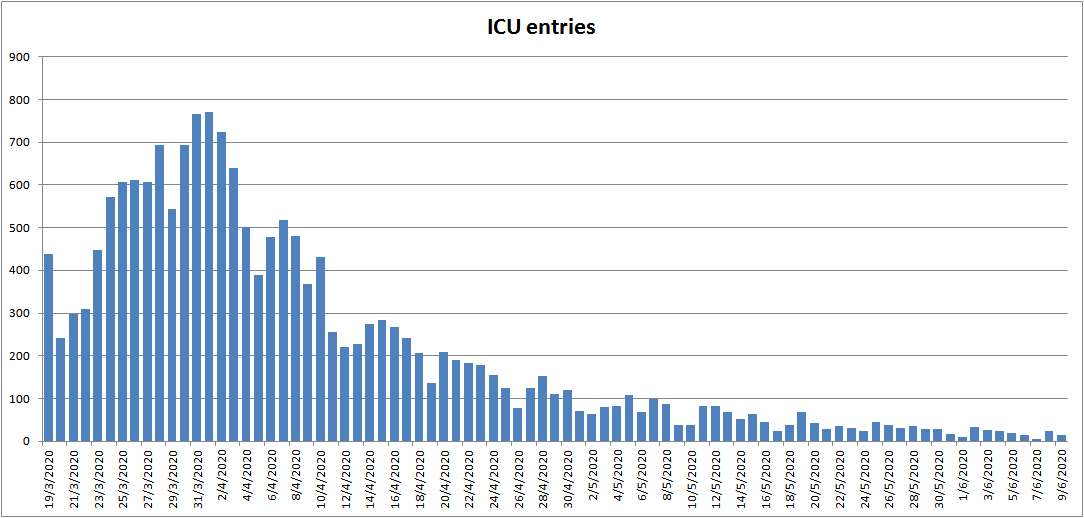
Hospital graphs:
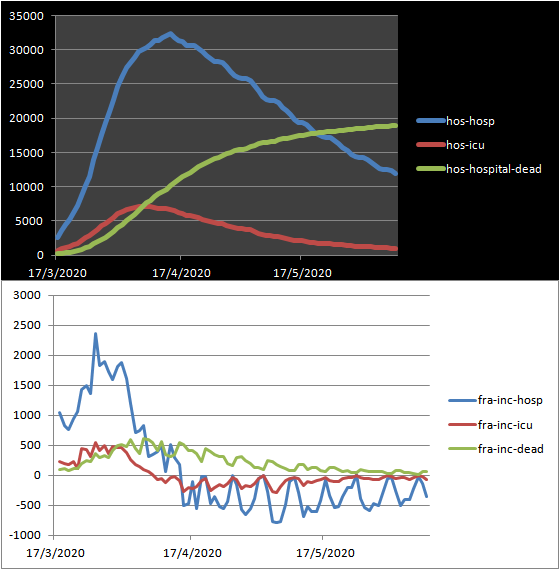
ICU entries:
French situation for the 09/06:
154591 confirmed cases + 403 in 24H
hospital:
11961 hospitalized -354 in 24 H (169 entries)
955 in intensive care -69 in 24 H (15 entries)
18912 dead + 53 in 24 H
Care homes:
37599 cases +194
10384 dead + 34
Total 29296 deaths +87 in 24H
Hospital graphs:
ICU entries:
Virginia unveiled its plan for reopening schools today for those in the education field and/or curious:
https://www.governor.virginia.gov/newsroom/all-releases/2020/june/headline-857292-en.html
as far as I understand it, schools will be able to open in the Fall while following social distancing guidelines (keeping students 6 feet apart [lmao], reducing classroom sizes, eating lunch in the classroom, etc.) staff will be required to wear masks; students will be encouraged to do the same. and then some students might opt to do everything entirely online.
a few districts have already shared some ideas about how they might proceed, though they've acknowledged they'll have to start later to adequately plan for all of this. one idea presented by one district that I actually don't hate is staggering the schedule so that one group of students attends on Mondays/Wednesdays, another on Tuesday/Thursdays, and Fridays are staff workdays.
tl;dr: it's a mess and they probably should've stuck with remote learning for the first semester
https://www.governor.virginia.gov/newsroom/all-releases/2020/june/headline-857292-en.html
as far as I understand it, schools will be able to open in the Fall while following social distancing guidelines (keeping students 6 feet apart [lmao], reducing classroom sizes, eating lunch in the classroom, etc.) staff will be required to wear masks; students will be encouraged to do the same. and then some students might opt to do everything entirely online.
a few districts have already shared some ideas about how they might proceed, though they've acknowledged they'll have to start later to adequately plan for all of this. one idea presented by one district that I actually don't hate is staggering the schedule so that one group of students attends on Mondays/Wednesdays, another on Tuesday/Thursdays, and Fridays are staff workdays.
tl;dr: it's a mess and they probably should've stuck with remote learning for the first semester
We'll notice it a whole hell of a lot earlier than last time. We probably have the same daily number of cases now as we really did weeks before we ever confirmed a single case.Thanks for posting the details. I'm still concerned and just facing the reality that we've gotta get back out there without knowing if/when there will be another spike/wave.
My Northern VA high school was extremely overcrowded when I went; checking now it looks like the teacher to student ratio for where I used to live is still about 15-18 students per teacher. I know I had classes with upwards of 30 kids in them sometimes. There's zero fucking way they can accommodate keeping students six feet apart in classrooms methinks.Virginia unveiled its plan for reopening schools today for those in the education field and/or curious:
https://www.governor.virginia.gov/newsroom/all-releases/2020/june/headline-857292-en.html
as far as I understand it, schools will be able to open in the Fall while following social distancing guidelines (keeping students 6 feet apart [lmao], reducing classroom sizes, eating lunch in the classroom, etc.) staff will be required to wear masks; students will be encouraged to do the same. and then some students might opt to do everything entirely online.
a few districts have already shared some ideas about how they might proceed, though they've acknowledged they'll have to start later to adequately plan for all of this. one idea presented by one district that I actually don't hate is staggering the schedule so that one group of students attends on Mondays/Wednesdays, another on Tuesday/Thursdays, and Fridays are staff workdays.
tl;dr: it's a mess and they probably should've stuck with remote learning for the first semester
in addition to that, young kids in particular are usually pretty jittery and like to get up and move around at the first opportunity. there's zero way to enforce it even if you can reduce the classroom sizes.My Northern VA high school was extremely overcrowded when I went; checking now it looks like the teacher to student ratio for where I used to live is still about 15-18 students per teacher. I know I had classes with upwards of 30 kids in them sometimes. There's zero fucking way they can accommodate keeping students six feet apart in classrooms methinks.
i'm curious to see what everyone's plan is for when someone in the school finds out they're infected. it's inevitable, and parents are probably going to start pulling their kids back out at that point.
Yeah, the Homestead race will have less than 1,000 people, all first responders and military folks. They should be able to keep everyone spread apart as that's way under capacity for the venue.
Don't know how many folks will be allowed in for Talladega yet. I would imagine a similar number (and it's a larger venue)

Coronavirus: more than a dozen US states see record high of new cases
Fourteen states and Puerto Rico see highest seven-day average of new infections, as restrictions to slow the spread are being relaxed
 www.theguardian.com
www.theguardian.com
Presume this has been discussed but this seems worrying.
Thanks for this. Twitter and the general scientific illiteracy of journalism mean that all the context is lost. WHO are right to say that we don't know, and to give the evidence for different possibilities. But that takes a few minutes to explain and we need one sentence so we get bullshit tweets about how "WHO experts say that 16% percent of the time it rarely happens 40% of the time"Regarding the WHO and asymptomatic transmission.
I have listended to both yesterday's and today's explanation. And there is a clear distinction they made: Contract tracing and models.
While doing contact tracing it seems rare that an asymptomatic person could spread the virus. This is what several countries seem to report and based on actual contract tracing data. That information is not perfect, but at least helpful as an additional data point. Contract tracing asymptomatic persons seems to be a pain honestly and probably a reason why there are not many studies yet.
On the other hand, there are models that estimate the proportion of asymptomatic transmitters at 40%, with a high range of uncertainty.
And they mentioned, yesterday and today, that the data is not conclusive and that they cannot fully answer the question and need more research.
And that's being done.
Singapore has "reduced" their lockdown, as we are down to 0-6 local cases a day and 200-400 dorm cases. Many businesses are still closed and I'm not sure I can go to the office again this year. School has reopened, although every-other-week for most, and regardless of if you're going shopping or not, you must wear a mask outside of your residence. Even if you're at school, even if you're getting a haircut, even if you're sitting at your work desk. The mask is the law. (Swimming, of course, is still not possible)
So to give north america one quick example of what this means: Let's go to Starbucks!
- Go to the mall with the Starbucks
- Scan to check-in (app)
- Go to the starbucks
- Scan to check-in (app)
- Buy the drink as usual
- You can't drink it! So you must take it home.
- Check out of the starbucks (app)
- Check out of the mall (app)
Of course, the two countries are negotiating what to do - and we already have fast-track flights to China - but the policies for C19 and the money invested are quite different. Malaysia is not "poor" but they are much larger and less well tracked than Singapore, so neither side wants to break their containment strategy for the other. (Singapore's strategy is very public, very hard data, Malaysia is...well, more difficult to track.)
Anyway, as you can imagine delivery is extremely popular right now and the cab services are basically splitting time with package delivery now also.
Idk, these increased numbers aren't even close to what NY or NJ were experiencing, and it's not going up exponentially. The "most hospitalizations since start" in Texas is about the same as current ones in NJ and Texas has 3x the population.In the greater NYC area, the virus is dieing out rapidly (look at my post right below yours) and we have the proper testing infrastructure in place now. The risk isn't completely eliminated but its minimal. Now if you were in Texas or Florida I'd be REALLY worried.

Two Genetic Regions Linked with Severe COVID-19
In a genome-wide association study, variants in both the ABO blood group locus and a cluster of genes on human chromosome 3 are more common among COVID-19 patients with respiratory failure than in the general population.
 www.the-scientist.com
www.the-scientist.com
It's not yet clear why some people infected with SARS-CoV-2, the virus that causes COVID-19, get really sick, while others have only mild symptoms. There's some evidence that chronic health conditions—such as hypertension and diabetes can play a role, and scientists know that people's genes can influence how their bodies react to other viruses. In a preprint posted to medRxiv on June 2, researchers describe a genome-wide association study (GWAS) of samples from 1,610 hospitalized patients with COVID-19 and 2,205 healthy controls. The authors identified variants in two regions—the locus that encodes blood type and a multi-gene cluster on chromosome 3—that were linked to respiratory failure during SARS-CoV-2 infection.
"We know that people vary in their susceptibility to infectious diseases, and variation in the human genome plays a . . . role in that susceptibility," Charlotte Houldcroft, who studies interactions between viruses and hosts at the University of Cambridge and was not involved in the work, writes in an email to The Scientist. "A genome-wide association study is a very good way to look at lots of variants across the human genome all at once, without a preconceived idea about which genes might be involved."
One region the authors identified is the locus that encodes blood type. They found that people with blood type A were at a higher risk for respiratory failure, while blood group O seemed to be protective. The odds for those with blood type A to be hospitalized with severe respiratory symptoms were nearly 1.5 times the odds for people with other blood types. And those with type O had about two-thirds the odds of being hospitalized as those with other blood types. This analysis echoes preprint findings from patient datasets collected in China and New York, which Franke says makes the research team more confident that it's a real association.
The other genomic region the researchers identified shows up on the human chromosome 3 and contains several genes of interest. One is SLC6A20, which encodes an amino acid transporter that interacts with ACE2, the main receptor that SARS-CoV-2 uses to get into human cells. Two other genes in this cluster encode immune system–related chemokine receptors: the C-X-C motif chemokine receptor 6 and the CC-motif chemokine receptor 9. Both proteins play a role in T-cell differentiation and recruitment during influenza viral infections. This region also shows up in publicly available results from the COVID-19 Host Genetics Initiative, which gives it weight, the authors write.
"Chemokine receptors are important in many manifestations of multiple diseases, so that's interesting," says Benjamin Fairfax, a geneticist at the University of Oxford who did not participate in the study. He adds that the SLC6A20 association is also intriguing because of the interaction with ACE2, but that the findings for both the chromosome 3 and blood group loci need to be replicated to give more insight into the underlying biological mechanisms of the disease.
So here's an interesting tid-bit... maybe I am overthinking it....
I live in New Jersey, where the first case of Coronavirus was documented in March.
In early January I became extremely ill, the worst I've ever been sick in my entire life by far. Fever, diarrhea, weakness, body aches, loss of appetite, shortness of breath; these symptoms lasted over a week but my cough and shortness of breath continued for nearly 8 weeks. After about 2 days of these symptoms I went to see my doctor and was tested for the flu because I had all the usual symptoms, I waited a few days and the test result came back as negative for influenza. I thought this was very suspicious, but I continued to take my medication and eventually recovered.
I would love to know if is at all possible that back in January someone in NJ could have had the COVID19 virus. Many of my coworkers also became very sick around the same time, one even with a dangerous case of Pneumonia. Also my mother in law who I was in contact with also had a case of Pneumonia shortly after I recovered.
I tried to reach out to Hackensack hospital because they are performing blood tests for recovered patients. Apparently there are antibodies in the blood that can be used to help other patients recover. Sadly because I never tested positive for the virus (tests were not being done in January), I cannot receive this blood test nor donate blood to help patients recover...
I guess I'll never really know for certain.
Bumping my own post from April....
Anti body tests became available to everyone (in NJ at least). I got tested Monday and just got the call that I have tested positive for Anti Bodies which means I had the virus just as I suspected.
I had this in fucking January....
Of course, a perfectly reasonable headline from WHO's statement is "WHO Suggests Contact Tracing Is Highly Effective For Suppressing Coronavirus Spread" but that requires some mild analysis from the editor so forget it.Thanks for this. Twitter and the general scientific illiteracy of journalism mean that all the context is lost. WHO are right to say that we don't know, and to give the evidence for different possibilities. But that takes a few minutes to explain and we need one sentence so we get bullshit tweets about how "WHO experts say that 16% percent of the time it rarely happens 40% of the time"
Also (referring to Minnesota):
While I'd be shocked if absolutely nothing shows up in the next two weeks, I feel like if we were really in the shit, something would have bumped already? In MN, just enough time has passed for two waves of symptomatic infections and plenty of time for some kind of hospitalization increase.
Idk, this thing is just super weird.
Last edited:
So yesterday, Chilean Government announced yet another change in methodology (third in two weeks) when reporting the death toll. Announced only 19 with this new methodology, which no one believed since we had 90+ daily.
Reports now say that said methodology actually indicates that the 100+ deaths daily was already surpassed a couple of weeks ago, so it's even more mindblowing how they NOW used said methodology because it reported 19.
They are messing with the number, making people get confused about the situation we are in, and just a total and complete fuck up.
Source, in spanish

 www.adnradio.cl
www.adnradio.cl
Reports now say that said methodology actually indicates that the 100+ deaths daily was already surpassed a couple of weeks ago, so it's even more mindblowing how they NOW used said methodology because it reported 19.
They are messing with the number, making people get confused about the situation we are in, and just a total and complete fuck up.
Source, in spanish
Cambio en metodología de conteo reveló que Chile superó los 100 fallecidos diarios por coronavirus a fines de mayo
El ajuste desde el Ministerio de Ciencia y Tecnología da cuenta de una cantidad de muertes superior a las informadas oficialmente.
www.adnradio.cl
Bumping my own post from April....
Anti body tests became available to everyone (in NJ at least). I got tested Monday and just got the call that I have tested positive for Anti Bodies which means I had the virus just as I suspected.
I had this in fucking January....
Wow. Glad you now know. We're in NJ and my wife / daughter had "pneumonia" out of nowhere in January. My wife is a teacher and has a rock-solid immune system but she was laid out for days. I also had a mild dry cough that lingered for weeks... whereas for allergies and sinus infections I usually have a wet cough. We all tested negative for the flu. Really want to get the antibody test now.
How did you go about signing up / getting the test?
Where did you get tested?Bumping my own post from April....
Anti body tests became available to everyone (in NJ at least). I got tested Monday and just got the call that I have tested positive for Anti Bodies which means I had the virus just as I suspected.
I had this in fucking January....
Of course, a perfectly reasonable headline from WHO's statement is "WHO Suggests Contact Tracing Is Highly Effective For Suppressing Coronavirus Spread" but that requires some mild analysis from the editor so forget it.
Also (referring to Minnesota):
While I'd be shocked if absolutely nothing shows up in the next two weeks, I feel like if we were really in the shit, something would have bumped already? In MN, just enough time has passed for two waves of symptomatic infections and plenty of time for some kind of hospitalization increase.
Idk, this thing is just super weird.
I think it's really just that outdoor spread is a very minimal risk. Indoors is where the danger is.