They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
That's honestly not bad. I expected more, but it's still shit.
They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
Here's someone a lot cleverer than me explaining why you shouldn't be so worried about that:
Long-Term Effects of COVID-19 Vaccines: Should You Be Worried?
Lately I’ve observed a lot of worry about long-term effects from COVID-19 vaccine candidates, which I fully understand. Almost. This seems…edwardnirenberg.medium.com
It has been used in humans for 10 years? Somehow I doubt that but if you can show the receipts Ill accept it.The mRNA part of it has been in testing and development for nearly 10 years. Beyond that we know quite a bit, most effects happen within the first 2-3 months of a vaccine, and we're well past that for early trials.
It should do, as a lot more safety measures were added in as a result of the issues then.
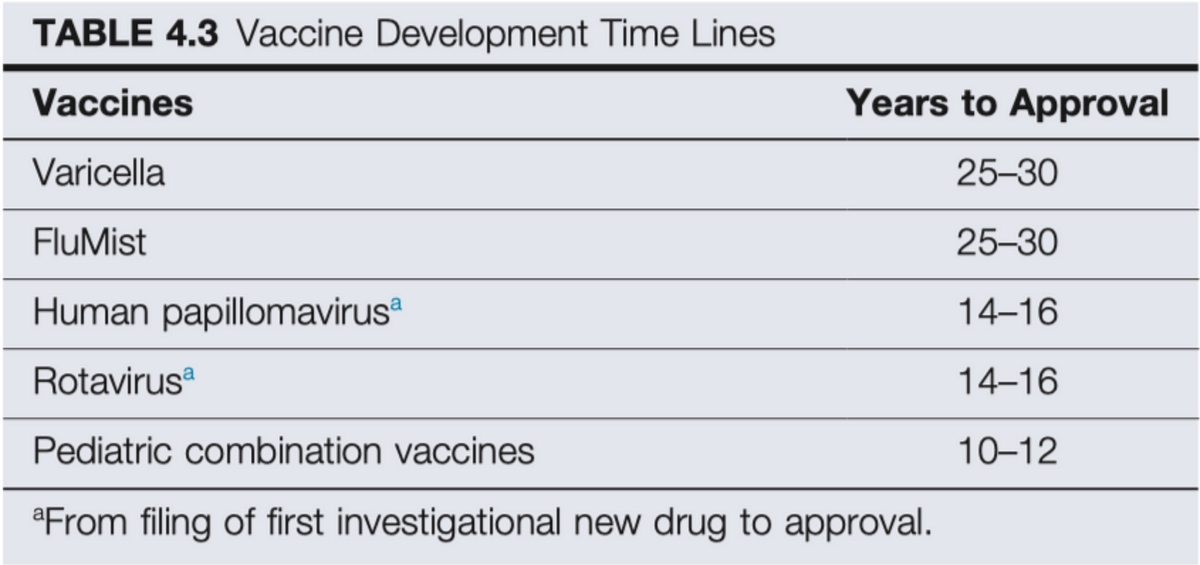
I am still nervous at all these vaccines getting approved without any knowledge of long term side effects. The previous fastest vaccine in history took four years, doing these in less then one is concerning imho.
It has been used in humans for 10 years? Somehow I doubt that but if you can show the receipts Ill accept it.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Plus the fact that they have to grow the virus to harvest the needed components as well. With an mRNA vaccine, they can just literally build the mRNA of an existing DNA segment template. They can build JUST what they need instead of harvesting it from a culture.There's been lots of commentary about that. Two of the major reasons for the delay in vaccines are lack of funding and red tape. Neither are a problem here.
Happy to help. :) There's also this, on a similar topic from the same author:Thanks for this. This is exactly what I've been wanting to see. A data driven break down of why we can trust a rushed production vaccine. This is great.
 edwardnirenberg.medium.com
edwardnirenberg.medium.com
To be fair, it seems like Oxford hired clowns and morons to manage their study and interpret their results. That helps keep costs low.They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
They are more expensive to make. Pfizer is selling their at $20 per dose.They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
There was one, it died quiclky.I think it would be really valuable to open up a "Vaccine Q&A" thread in here to act as a resource for people to be informed. Vaccine hesitancy is especially real for COVID-19 and I feel like a lot of people's concerns could be addressed if they were able to ask their questions in a safe environment
Biontech has already been conducting human trials for their mRNA based cancer vaccine since 2017.It has been used in humans for 10 years? Somehow I doubt that but if you can show the receipts Ill accept it.
Can someone explain the science behind this to me?Looks like the endpoint results are:
196 cases - 185 placebo (94.4%), 11 vaccine (5.6%) - so 94.1% relative reduction in the vaccine group
30 severe cases - all 30 in placebo
1 death - in the placebo group
And a suitably diverse mix of people in the trial, too:
(Note that where it says 'in the final analysis', it means that 33 older adults and 42 BAME people were in the 196 cases)
For usable results, they had to wait until a certain number of people in the test got COVID. In this case it looks like they got 196 cases.Can someone explain the science behind this to me?
Aren't we testing the effectiveness of the vaccine? And only 11 there were given the vaccine and 185 weren't? I genuinely don't know how this works, feels like I'm missing something.
15,000 people were given the vaccine.. After they'd received both jabs, 11 of them developed Covid-19, no serious cases, no one died.Can someone explain the science behind this to me?
Aren't we testing the effectiveness of the vaccine? And only 11 there were given the vaccine and 185 weren't? I genuinely don't know how this works, feels like I'm missing something.
This is a really helpful blog post and the thing that it boils down to for me is this:Here's someone a lot cleverer than me explaining why you shouldn't be so worried about that:
Long-Term Effects of COVID-19 Vaccines: Should You Be Worried?
Lately I’ve observed a lot of worry about long-term effects from COVID-19 vaccine candidates, which I fully understand. Almost. This seems…
Consider the ever-expanding litany of long-term consequences we are tracing to COVID-19 infection- consequences which are not uncommon. My personal view is if this is such a risk from a vaccine for COVID-19, it would likely still be worth getting because the risks posed by infection will still be far greater.
In much the same way as we don't fully know how long immunity lasts after infection, we don't know here either. Tests so far show that the immune response in those given the vaccine is at the same level or higher than those naturally infected, so it should be at least as good as those who recover from the disease. However, it's not known for certain, as enough time hasn't elapsed yet.
They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
That makes more sense, thanks!15,000 people were given the vaccine.. After they'd received both jabs, 11 of them developed Covid-19, no serious cases, no one died.
15,000 people were given the placebo.. After they'd received both jabs, 185 of them developed Covid-19, 30 serious cases, one died.
I've tweaked that initial post now so hopefully it's a bit clearer!
These things cost serious money to develop. It's not greed. Unless you think Moderna should eat a loss out of principle.They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
Well, not really. They are two totally different technologies. Moderna's is actually one of the first of its kind, to say nothing of the merits of the AZN/Oxford vaccine.
Moderna could charge $4 and just eat whatever loss it would need to, but it is important to note that Moderna is a dramatically smaller, less liquid, and more thinly capitalized company than like a Pfizer or an AstraZeneca. The government should just pay for everything anyway.
Nurses are prio 1 normallyI hope my SO who is a nurse and has several risk factors can get it soon. Also my mom who needs to freaking stop going places.
They are charging $32 to $37 per dose. That's really shitty, especially when the Oxford one will only be charged at $4 per dose.
Greed.
Well, not really. They are two totally different technologies. Moderna's is actually one of the first of its kind, to say nothing of the merits of the AZN/Oxford vaccine.
Moderna could charge $4 and just eat whatever loss it would need to, but it is important to note that Moderna is a dramatically smaller, less liquid, and more thinly capitalized company than like a Pfizer or an AstraZeneca. The government should just pay for everything anyway.
I hope my SO who is a nurse and has several risk factors can get it soon. Also my mom who needs to freaking stop going places.

Pandemrix did not go through normal trials and was given immunity in the UK. They also used an oil adjutant they suspect of maybe triggering narcolepsy in a small amount of people. The evidence is not super conclusive. CDC says the link remains unproven.
More info on the subject here: buzzfeed.com/shaunlintern/these-nhs-staff-were-told-the-swine-flu-vaccine-was-safe
And here: https://www.statnews.com/2018/07/05/flu-vaccine-2009-pandemic-narcolepsy/
Fortunately, covid vaccines ARE going through trials to unmask precisely these kinds of problems. I'll feel much more comfortable taking my chances with a well-tested vaccine than stupid humans who can't use masks and insist on infecting me at every turn.
Plus, while it's relatively depressing to think about, you also have to take into account the fact that at least 5% of the US population will (or, perhaps its better to stay should) have some level of immunity due to being exposed to the virus itself.At 90% effectiveness, you really only need to vaccinate about 50% of the population to kick Covid's ability to spread. And even at 20-30% of the population, it wil be safe to open up with minimally intrusive measures.
My job requires me to be in a hospital and in clinics, in January. I won't be interacting with patients directly, but will have contact with medical personnel both directly, and indirectly. This will be on Military bases, so I wonder if I'd have a better chance of getting a vaccine than others? I've also already had Covid, so who knows.
Yes, and therein lies the rub. I have no qualms about the immediate/short-term efficacy of the vaccine and the trial findings thus far suggest no short-term serious side effects take place. From a public health standpoint, taking into account the nature of coronaviruses in general (and the long-term efficacy of prior vaccines for this type of virus) I wonder about the efficacy of a COVID-19 vaccine over the long-term and the logistics of delivering many multiples of vaccinations. If it's a yearly thing like influenza, then I suspect all will be well. If it's a few months, there will be issues. Unfortunately the only thing we can do is wait and see.In much the same way as we don't fully know how long immunity lasts after infection, we don't know here either. Tests so far show that the immune response in those given the vaccine is at the same level or higher than those naturally infected, so it should be at least as good as those who recover from the disease. However, it's not known for certain, as enough time hasn't elapsed yet.
Indeed, although this will be ignored in vaccination policies.Plus, while it's relatively depressing to think about, you also have to take into account the fact that at least 5% of the US population will (or, perhaps its better to stay should) have some level of immunity due to being exposed to the virus itself.
Looking solely at public healthcare, probably not because you're not a healthcare worker. Military, I'm not sure.My job requires me to be in a hospital and in clinics, in January. I won't be interacting with patients directly, but will have contact with medical personnel both directly, and indirectly. This will be on Military bases, so I wonder if I'd have a better chance of getting a vaccine than others? I've also already had Covid, so who knows.
tbh i am on the fence i will get it but i feel i should wait a certain amount of time first. to observe the effects before taking the plunge because a rushed vaccine can be detrimentalYeah, to his point though - this is new technology. I am not saying we shouldnt try to exit this nightmare as fast as possible. But still, we dont know much.
At the moment, there are too many strains to make it interesting. Can't get 80-100 strains into one vaccine. There is also little monetary incentive to invest in the testing because a vaccine costs a lot of money to test, and if you can't cover every type of cold, people are not going to buy it.A related question. Since they are using this for a coronavirus and using the mRNA method does that mean once COVID-19 has settled down that we could possibly have vaccines against cold viruses for the first time in human history? That would be awesome!
Stable at standard refrigerated conditions of 2° to 8°C (36° to 46°F) for up to 30 days within the 6-month shelf life.
The main challenge is production, since Moderna is a relatively new company and lacks the infrastructure of Pfizer.
I'm glad minorities made up a good amount of their test group. The side effects do seem a bit rough though. But it's better than dying.
Based on what these numbers mean (ie the 94% comes from cases developed as the denominator, and not number of people in the trial as the denominator), I'm guessing they weren't purposely exposed to covid. How do they account for people who got either and just stayed home?15,000 people were given the vaccine.. After they'd received both jabs, 11 of them developed Covid-19, no serious cases, no one died.
15,000 people were given the placebo.. After they'd received both jabs, 185 of them developed Covid-19, 30 serious cases, one died.
I've tweaked that initial post now so hopefully it's a bit clearer!
Headache, fatigue, sore arm and potentially high fever the day after getting it. About 1 in 10 have side effects.
They don't. You need a minimum amount of infections to open up the trial. If all your participants stayed home and didn't get Covid, testing would take a lot longer. The spread of Covid is to thank for the fast results. Vaccines for SARS and MERS failed because it was impossible for the placebo people to get sick. If there had been a cure or an effective treatment for Covid, they would have done direct infection but that is not ethical when there is no treatment.Based on what these numbers mean (ie the 94% comes from cases developed as the denominator, and not number of people in the trial as the denominator), I'm guessing they weren't purposely exposed to covid. How do they account for people who got either and just stayed home?
Based on what these numbers mean (ie the 94% comes from cases developed as the denominator, and not number of people in the trial as the denominator), I'm guessing they weren't purposely exposed to covid. How do they account for people who got either and just stayed home?